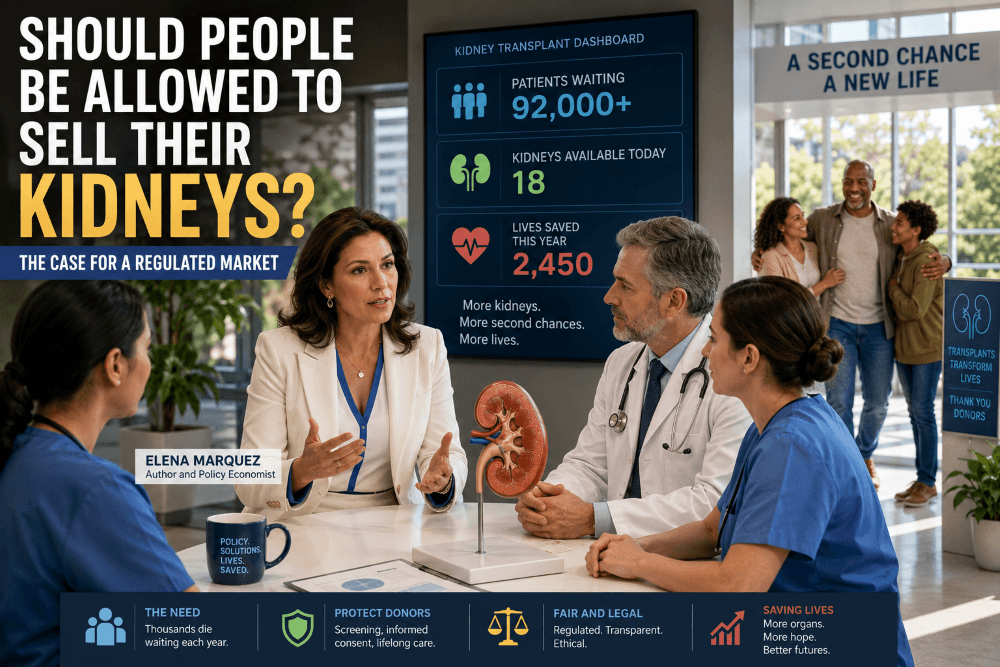
Every year, thousands of people die while waiting for a kidney transplant. A regulated kidney market could increase the supply of kidneys, reduce waiting times, and save lives while protecting donors through strict medical oversight. The question is uncomfortable, but it deserves serious discussion.
For decades, most countries have prohibited the sale of human kidneys while allowing compensation for other forms of biological donation, such as sperm, eggs, and, in some jurisdictions, plasma. Is there a principled reason for this distinction, or are we allowing preventable deaths because of an outdated moral intuition?
The Human Cost of the Kidney Shortage
Kidney failure is not a rare condition. Thousands of patients spend years on transplant waiting lists while undergoing dialysis several times each week. For many, a compatible kidney never arrives.
The consequences are tragic.
Every year:
- Thousands of patients die before receiving a transplant.
- Many others become too sick to qualify for surgery.
- Families watch loved ones endure years of declining health despite the existence of a treatment that could dramatically improve their quality of life.
The shortage is not caused by a lack of medical knowledge. Surgeons know how to perform kidney transplants. The problem is simply that there are not enough donated kidneys.
Why a Regulated Kidney Market Deserves Consideration
Markets exist because incentives matter.
When society needs more food, housing, or medicines, we rely on incentives to encourage production. Human organs are understandably different, but the basic economic reality remains the same: when demand greatly exceeds supply, shortages occur.
A regulated kidney market would not be an unregulated marketplace where brokers exploit vulnerable people. Instead, it could operate under strict government supervision with safeguards such as:
- Comprehensive medical screening.
- Independent psychological evaluation.
- Fully informed consent.
- Fixed compensation rather than bidding wars.
- Lifetime medical monitoring for donors.
- Criminal penalties for coercion or trafficking.
The objective would not be to commodify people. It would be to create a legal, transparent system that increases the supply of kidneys while protecting everyone involved.
We Already Compensate Other Biological Donations
Many people react negatively to the idea of paying kidney donors, yet society already accepts compensation for other biological materials.
Examples include:
- Sperm donation.
- Egg donation.
- Plasma donation in some countries.
- Participation in clinical research studies.
These arrangements recognize that people may voluntarily accept inconvenience, discomfort, or medical risk in exchange for compensation.
Kidney donation involves greater risks and therefore requires much stronger protections. But the existence of those risks does not automatically answer the ethical question. Instead, it raises another one: if adults can make informed decisions about many other medical procedures, why should kidney donation be treated differently under a carefully regulated system?
A Better Alternative Than the Black Market
Prohibiting compensation has not eliminated the demand for kidneys.
Around the world, illegal organ trafficking still exists, with few protections for donors or recipients. Wealthier patients sometimes travel abroad seeking transplants through medical tourism, while those with fewer financial resources often remain on waiting lists with no alternatives.
A transparent legal framework could reduce incentives for illegal markets by moving donations into licensed hospitals where medical standards, informed consent, and long-term follow-up are mandatory.
The Economics Matter Too
Dialysis is an extraordinary medical achievement, but it is also expensive. For patients covered by traditional Medicare, the annual cost of care averages $90,000 to $98,000 per year per patient. Outpatient dialysis spending for private payers routinely ranges from $150,000 to over $238,000 per year per patient.
The total estimated cost for a kidney transplant with a living donor sits around $446,800.
Governments and insurance systems often spend substantial sums each year to keep patients alive while they wait for a transplant. Those costs can continue for many years.
Although a regulated compensation program would require public funding or insurance reimbursement, policymakers should compare its cost with the ongoing expense of long-term dialysis, repeated hospitalizations, and the broader economic consequences of chronic kidney disease.
A successful transplant can restore health, reduce long-term treatment costs for many patients, and allow many recipients to return to work and participate more fully in society. Whether compensation programs would reduce overall healthcare spending depends on their design, but the comparison deserves careful consideration rather than dismissal.
The Ethical Objections
The strongest objection is that paying for kidneys could pressure financially vulnerable people into becoming donors.
That concern should not be ignored.
However, banning compensation also has ethical consequences. Every year, patients die because no kidney becomes available.
Rather than asking whether paying donors feels uncomfortable, perhaps the more important question is whether it is ethical to maintain a system that predictably leaves thousands of patients without life-saving treatment.
The answer may not be a completely free market. It may instead be a tightly regulated system with independent oversight, mandatory counseling, standardized compensation, and lifelong healthcare protections for donors.
Is It Fair That Only the Wealthy Have More Options?
Access to healthcare is often unequal.
Patients with greater financial resources may have more opportunities to seek treatment in other countries or explore additional medical options, while lower-income patients are more dependent on domestic waiting lists. Although international transplant practices vary widely and ethical standards differ by country, disparities in access remain an important concern.
A well-designed domestic compensation program could expand the legal supply of kidneys, reducing waiting times for all eligible patients regardless of income.
The Real Ethical Question
Discussions about organ donation often focus on whether kidneys should be bought and sold.
Perhaps that is the wrong question.
The better question is this:
Is it ethical to let people die waiting for kidneys when willing donors could legally save them under a carefully regulated system?
Reasonable people will disagree on the answer.
But given the thousands of lives at stake, this is a debate worth having—not with slogans or emotional reactions, but with evidence, compassion, and a willingness to rethink long-standing assumptions.
Frequently Asked Questions
Would a regulated kidney market eliminate organ shortages?
It might significantly reduce shortages, although the exact impact would depend on donor participation, regulatory design, and public acceptance. Most experts agree that increasing the supply of kidneys is a central challenge.
Would selling a kidney be legal under this proposal?
Only within a tightly regulated medical framework. The proposal is not for an unrestricted market but for government oversight, informed consent, medical screening, and long-term donor care.
Would poor people be exploited?
This is the primary ethical concern raised by critics. Supporters argue that strong safeguards—including independent counseling, fixed compensation, and protections against coercion—could reduce that risk while giving adults the freedom to make informed choices.
Could a regulated kidney market reduce healthcare costs?
Potentially. Kidney transplants often reduce the long-term need for dialysis and repeated hospitalizations, though the financial impact would depend on how a compensation system is designed and funded.
Leave a Reply